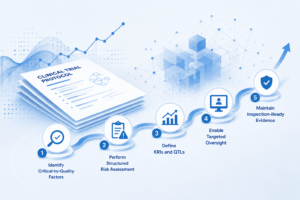
When quality breaks down in a clinical trial, the cost isn’t limited to rework. It can slow enrollment, delay regulatory submissions, strain site relationships, and ultimately postpone getting treatments to the patients who need them.
This is why quality is not simply a compliance exercise; it is a strategic performance driver. The organizations that “design quality in” early are the ones that avoid costly disruptions later.